Sexual Dysfunction
The Brain-Body Connection
Ed. Balon, R.
©Copyright 2008 S. Karger AG, Basel
If you want an up-to-date academic guide to sexual dysfunction, then definitely don't listen to me. You should turn to the leaders in the field. You can refer to the textbook pictured above and edited by Balon. I'm sure it will answer any question that is answerable in light of our current knowledge.
If you want an "off-the-cuff" and entertaining guide to sexual dysfunction, then feel free to continue.
•
According to my therapist, the predicament that I described earlier in regards to all the nurses rejecting my romantic advances would not technically be described as sexual dysfunction. My therapist goes on to describe some sort of personality thing but I won’t bore you with all that here. The point is that sexual dysfunction is an unusual problem because it is relatively easy to fix and, yet, it is a huge problem.
Ignorance and selfishness are the only real problems with regards to sexual dysfunction but these two problems can cause all the other problems to go unresolved.
For example, a woman is not able to achieve an orgasm during coitus. This is called anorgasmia. Well...a tongue or a finger or a play toy or a visual aid or incense or body oil or music or simply better technique could easily solve this problem. The problem goes unresolved and the guy complains to his buddy that his woman is "frigid."
All this guy needs is a little education about proper technique and maybe some verbal feedback from his partner and, oh yeah, he has to give a damn about pleasing her.
Let's talk about some other things that are frequently referred to as sexual dysfunction. Wait a minute…I have an idea. Why don't we throw the term "sexual dysfunction" in the trash can and find a new way to talk about this stuff. Let's call it "change in sexual function." Yes, that's much better. That eliminates any value judgment attached to the mere description of sexual difficulties.
The term "change in sexual function" has several additional advantages. First, it's a more accurate way to describe the problems we are talking about. Second, it incorporates the full range of changes that might occur rather than just the ones that are bad. Finally, a change seems to infer that there can be more changes. We can respond to a change in function and make a change ourselves and create something new and better. I always like to define a problem in a way that points to a possible solution.
OK, let's talk about some "changes" in sexual function.
Suppose a man is in the upper or lower 5% with respect to the size of his penis. Sex will be more difficult but as long as he is capable of ejaculating and willing to learn some technique then there should be no problem. In fact, because the man is compensating for a tiny or an enormous penis he might learn some clever extra-penetration techniques to please a woman. Who knows, he could become the most popular guy among his friends.
I know a guy who recently divorced his wife and married a younger woman. His complaint was, "My ex-wife was boring and never wanted to have sex."
After the divorce she went to a psychiatrist and got her depression treated and is now in a very happy relationship and having tons of sex. My friend is irritated with the little girl he married and he rarely has sex with her. Go figure.
All he had to do was to care about his wife and he would have discovered that the problem was depression. If he had helped her get treatment, then he would still be in a good relationship with a mature woman and he would be having sex all the time.
The problem was not depression. The problem was a nasty combination of selfishness and ignorance.
•
What about Levystien's favorite dysfunction...I mean change...no...In this case, I think dysfunction is more accurate?
Oh, yeah. My favorite sexual dysfunction is one that isn't on the official list. It's one that some sophomoric sex therapists fail to even talk about. It is probably the most obvious dysfunction that there is but virtually nobody ever thinks about it or talks about it. It's a true dysfunction in that there is little you can do to correct it. It just is and you have to accept it.
Fortunately, there is a cure. The cure is very simple; you must find a new partner. The good news is that finding a new partner is potentially a 100% effective treatment. OK, here it is:
You are not in Love!
The problem here is that one or both partners are simply not feeling a strong sexual attraction. For whatever reason we are turned on by some people and turned off by others. Think about it. It's different with Pamela Anderson than it is with Rosie O'Donnell, right?
I know plenty of girls who had sex with lots of guys and never had an orgasm. They all thought they were frigid until they had sex with me. Actually, I only know one but you get my point.
Just because a woman fails to have an orgasm with Pee Wee Herman does not mean she won't cum 5 times with Mel Gibson.

I'm not even talking about how objectively gorgeous your partner is. I'm really talking about how good a match you are. If you are with the right person then there is a greater likelihood of a fantastic orgasm. Not that there can't be a sexual dysfunction that needs to be overcome, even with your perfect match, but the more perfect the match is the better the sex will be.
For all you guys out there who think too highly of themselves, here is a little something to ponder. Do you really want to have sex with Pamela? I mean, she will do it but she may not have an orgasm. If she does have an orgasm, it probably won't be as good as the one she had with Tommy Lee. You will likely ejaculate prematurely and you will feel she is judging you negatively the entire time. You might even catch her glancing at the clock while you are in mid stroke. Seriously, do you really want to have sex with this woman? OK, yes, but you understand what I am saying, right?
•
Here is an interesting aside; just because you are not in love does not mean you are failing to fully satisfy your lover. For example, what would you do if you were a homosexual man but married to a woman? You might platonically love this woman but you are not romantically attracted to her. Don't you think that you might work very hard to fully please her because your greatest fear is that you will be detected?
I don't mean to strike fear into the hearts of all you ladies out there who are married to fabulously unselfish lovers. I hope you won't start mistrusting them and following them around to see if they have a homosexual lover. What would be the purpose of doing that? Suppose you caught him with a guy? Are you going to be willing to give up the great sex? If I were you I would just forget about it and count my blessings.
•
In the previous chapter there was a list of changes in sexual function that may need to be overcome in order to have a better sex life. Here is a repeat copy of that list so we can reference it easier as we continue to discuss items on the list.
Changes in Sexual Function
Male
Erectile dysfunction
Female
Painful intercourse
Anorgasmia
History of rape
Childhood sexual trauma
Both
Chronic medical condition
HIV+
Psychiatric disorders
Lack of time and energy for sex
Painful intercourse? What is this doing on the list? Is that even possible? It certainly seems like a contradiction in terms to me unless, of course, we are speaking about relations with Rosie O'Donnell. OK, I'll leave Rosie alone from this point on, probably not, but what is painful intercourse?
The official funny name for it is dyspareunia (pronounced “dis-pair-une-ee-ah”). It has probably never occurred to you but lots of female conditions can become painful upon intercourse. The most common causes of painful intercourse are prolapsed uterus, fallen bladder, ovarian cyst, adhesions, fibroids, endometriosis, and intestinal conditions. Should your woman experience dyspareunia you should get her to a doctor. You should report that you probed her with a long and erect instrument and found that she experienced pain. Well, that's what you did.
You will have actually done her a service and the problem can almost always be corrected. She may even have a cancer that you just discovered. If you save her life then I am thinking there will be a lot of good sex in your future.
If the pain is surface tenderness rather than pain on deep penetration then it is more likely to simply be an infection (viral, bacterial, or yeast), a dermatological condition such as squamous hyperplasia or lichen sclerosis, a partially intact hymen, inadequate lubrication, or simply a cut.
There is one condition that can cause the vaginal musculature to contract sharply and painfully upon attempted penetration. This condition is fairly rare. It is called vaginismus and is likely related to previous trauma. Contrary to popular belief, most causes of dyspareunia are not psychological but this one probably is.
Finally, there is a rare type of pain with intercourse that Levystien causes on a frequent basis. This one can produce pain after the man is lying next to the woman and breathing hard or, in a lot of cases, already asleep. The woman may actually enjoy this form of dyspareunia and not seek treatment.
This particular cause of dyspareunia does not have an official name. Therefore, I have decided to casually refer to it as Levystien Contractions (LC). LCs can occur after a woman has experienced intense or repeated orgasms. It seems that uterine contractions produced in this way may last for some time after the man is finished and could be so severe as to be painful. (Believe me, they don't complain.)
Actually, there is one more that I forgot about and this one is actually somewhat common and it is hilariously funny. Some women are actually allergic to semen. Imagine that! Some women have even gone into anaphylactic shock after intercourse. Sorry, I guess that isn't very funny.
Actually, this one is not funny at all. In fact, a semen allergy is kind of scary. I mean, how could I distinguish anaphylactic shock from the normal post-coital screaming and flailing about that I usually elicit.
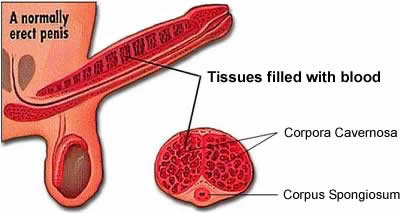
Erectile dysfunction (ED) used to be called impotency until they came up with a treatment and the name changed to ED. Similar to dyspareunia, the cause of impotency has traditionally been assumed to be largely psychological. Although the cause of impotency in men is more frequently psychological compared with the cause of dyspareunia in women, real physiology and not psychology is usually the culprit.
Common physiological causes of erectile dysfunction include:
- Heart disease
- Atherosclerosis
- High blood pressure
- Diabetes
- Obesity
- Parkinson's disease
- Multiple sclerosis
- Hypogonadism
- Peyronie's disease
- Surgeries or injuries
- Prescription medications
- Tobacco
- Alcoholism and drugs
One additional cause is rather interesting. It is bicycle riding. Prolonged riding can put pressure on the pelvic nerves and temporarily cause erectile dysfunction.
All men have occasional difficulty getting or maintaining an erection and many of the causes are reversible. So, how do you know if you have real ED? Also, is ED a medical problem that you should worry about outside of the bedroom?
If you suffer from a limp dick on more than a few occasions and there is no immediate explanation like alcohol, drugs, medications, or a really late night of partying or, I guess, a long bike ride…oh, yeah, or a really ugly girl, then I would recommend that the first thing you do is tape a piece of paper around the base of your penis at bedtime. Normally, you will have 4 or 5 erections at night during rapid eye movement sleep and this will break the paper. If the paper breaks, then you should see a psychologist. Otherwise, it means that there is a hemodynamic explanation.
If the paper does not break then you should see your family doctor because you may have a serious medical condition such as cardiovascular disease or diabetes or…well…I put a list up around here somewhere.
If the paper does break and you find that your ED is psychological then you should be happy because you are healthy and this is a pretty easy problem to fix. If you are lucky they might even send you to a sex therapist. I really don't know anything about that but is sure sounds cool.
One of the most common psychological reasons to have impotency is lack of confidence due to the idea that your member is too small. Since most male models that do pornography have large genitalia, or so I've been told, a lot of men tend to feel inadequate. In reality, the average male penis is two inches long fully erect. If yours is longer than this then you are clearly above average. (My grand pappy used to say, "If a lie hurts nobody and helps a lot of people, is it really a lie?")

Premature ejaculation (PE) is usually not caused by physiological problems. There are some exceptions including lifelong and genetically linked PE and, interestingly, opiate withdrawal but the vast majority of cases of PE are heavily influenced by psychological and environmental factors. In fact, one study showed that clinical PE is 87% more likely when a man's penis is in Pamela Anderson compared to when it is in Rosie O'Donnell. OK, I made that up, but I bet it's true.
Almost every man suffers PE during his first sexual experience as it takes some practice for a man to achieve control. Younger guys under the age of 30 tend to ejaculate faster but they can also repeat the performance sooner and more often. After some degree of expertise is achieved in the bedroom most guys are able to please their woman despite the latency period to ejaculation. Thus, PE is a common problem but it usually does not require medical intervention.
The diagnosis of PE is generally made only when one or both partners complain that repeated episodes are reducing their enjoyment of sexual activity.
Of course, psychiatric illness can be another cause of sexual dysfunction. The most common psychiatric cause is probably major depression. Decreased libido is actually an item on the check list to make the diagnosis.
Treatment for depression can also change sexual function. Selective serotonin reuptake inhibitors such as Prozac® can delay time to orgasm for both men and women. It should not be difficult to imagine why this would be called a "change in sexual function" rather than a "dysfunction." If you are an 18 year old man and you ejaculate in about 60 seconds, then some Prozac® might come in rather handy.
I really don't want to talk about rape and childhood sexual abuse but these things can certainly be a factor in a woman experiencing sexual dysfunction. You need to be sensitive to your woman having a history of sexual trauma. A lot of them do and they often don't talk about it. My advice is to treat all women as if they had been raped. Just be sensitive and caring, comprende?
The only reason that I am reluctant to talk about this stuff here is that I have no idea what it would be like to experience rape. I am trying to make jokes and I don't think that sexual abuse is an appropriate place to do that. Even Levystien can restrain himself on occasion.
Stress and relationship issues are a source of sexual dysfunction that most of us encounter from time to time, some of us more than others. I find that the best sex is a natural outgrowth of a healthy and mature relationship that is deep and profound on many levels. In order to achieve this you must have respect for your partner and for yourself. You must have conflicts that end with a productive resolution. You must fight fair and not simply lash out with insults. You must be able to agree to disagree. You must be sensitive to each other's feelings. You have to recognize each other's strengths and weaknesses so you can come together and create a couple that is stronger than either individual.
Nevertheless, even the best of couples will from time-to-time experience relationship stress. This should be anticipated and should not cause alarm. Remember, all you have to do is care about pleasing your partner and be willing to talk and listen and find a solution.
•
OK, let's finish this chapter on sexual dysfunction with some examples of really bad sex. Let's run through a few paradigms in which things just don't work out right for whatever reason.
1. Imagine that you are having sex with Pamela Anderson and you notice her glancing at the clock. You have a fear that your performance is inadequate and you lose your erection. Well, maybe that's not realistic. Let's move on to number two.
2. Suppose you are pumping an average looking woman and you can feel that your ejaculate is "in the shoot," so to speak, when she screams out, "You better wait until I cum first!!"
3. What if you take a woman to dinner and a movie and you get back to her place and she invites you in and you get undressed and she laughs and says, "Wow! Your pecker is really small."
Within about 20 seconds this comment would likely be followed by, "And now it's limp."
4. Suppose you are at dinner with a woman that you would like to have sex with. You are having casual conversation that is turning a bit provocative. She comments, "The last guy I dated had a really big dick."
5. You are naked and making love to a woman and she asks, "Am I beautiful?"
You respond, "Yeah, I guess so."
6. Here is the worst one of all. Unfortunately, it could possibly be the most common.
You stopped dating Beth and you are now dating Carol. You and Carol are hitting it off. There is a quaint little French bistro that you take her to and tell her all kinds of wonderfully romantic things. You buy her flowers on the spur of the moment as you walk down the sidewalk coming away from the bistro. She wilts as you tell her that you have never felt like this before. Then, after ripping each other's clothes off and starting to make love you exclaim in your most passionate voice, "Oh, Beeeeth!!"
I must confess, this last one is recounted from personal experience.
Sex Therapy